
Developing a Care Plan: Why It Matters
Developing a care plan is one of the most important responsibilities in nursing and healthcare practice. A care plan serves as a structured roadmap that identifies a patient’s health needs, establishes measurable goals, and outlines the nursing interventions required to achieve positive outcomes. Whether you are a nursing student completing an assignment or a practicing nurse providing patient-centered care, understanding the care plan development process is essential.
A well-developed care plan promotes continuity of care, improves patient safety, enhances communication among healthcare providers, and ensures that interventions are tailored to the patient’s unique needs.
What Is Care Plan Development?
Care plan development is the systematic process of creating an individualized plan of care based on a patient’s assessment findings. It involves identifying health problems, setting realistic goals, implementing evidence-based interventions, and evaluating patient outcomes.
The process follows the nursing framework known as ADPIE:
- Assessment
- Diagnosis
- Planning
- Implementation
- Evaluation
This structured approach helps nurses deliver organized, effective, and patient-centered care.
What Are the 5 Main Components of a Care Plan?
A nursing care plan consists of five key components:
1. Assessment
Assessment involves gathering comprehensive patient information.
Subjective Data:
- Information provided by the patient or family
- Symptoms, concerns, and personal experiences
Objective Data:
- Vital signs
- Laboratory results
- Physical examination findings
- Clinical observations
Accurate assessment forms the foundation for the entire care plan.
2. Nursing Diagnosis
A nursing diagnosis identifies actual or potential health problems based on assessment findings.
The diagnosis is commonly written using the PES format:
- Problem – The health issue identified
- Etiology – The underlying cause
- Signs and Symptoms – Evidence supporting the diagnosis
Example:
Impaired physical mobility related to left-sided weakness as evidenced by inability to bear weight and patient reports of pain.
3. Planning (Goals and Outcomes)
Planning involves establishing SMART goals that are:
- Specific
- Measurable
- Achievable
- Relevant
- Time-bound
Examples include:
Short-Term Goal:
Patient will maintain oxygen saturation above 95% during the next 8-hour shift.
Long-Term Goal:
Patient will independently perform activities of daily living within two weeks.
4. Nursing Interventions
Interventions are the nursing actions designed to achieve the established goals.
Examples include:
- Monitoring vital signs every four hours
- Administering prescribed medications
- Providing patient education
- Assisting with mobility exercises
- Implementing fall prevention strategies
Each intervention should include a rationale explaining why the action is necessary.
5. Evaluation
Evaluation measures the effectiveness of nursing interventions.
The nurse determines whether goals were:
- Met
- Partially met
- Not met
Based on the evaluation findings, the care plan may be revised to better address the patient’s needs.
What Are the 5 Stages of a Care Plan?
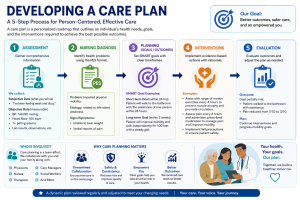
The five stages of a care plan correspond directly with the nursing process:
Stage 1: Assessment
Collect and organize patient information.
Stage 2: Diagnosis
Analyze assessment findings and identify nursing diagnoses.
Stage 3: Planning
Develop SMART goals and expected outcomes.
Stage 4: Implementation
Carry out nursing interventions and treatments.
Stage 5: Evaluation
Assess patient progress and modify the care plan as needed.
These stages ensure a systematic and evidence-based approach to patient care.
How Is a Care Plan Developed?
Developing a care plan begins with a comprehensive assessment of the patient. Nurses gather subjective and objective data to identify health concerns and prioritize patient needs.
Once sufficient information is collected, nursing diagnoses are formulated. SMART goals are then created to provide measurable targets for improvement. Evidence-based interventions are selected and implemented to support these goals. Finally, the patient’s response is evaluated, and adjustments are made when necessary.
Effective care plan development requires critical thinking, clinical reasoning, and collaboration among healthcare professionals, patients, and family members.
Why Care Plan Development Is Important
A properly developed care plan provides numerous benefits:
- Enhances patient safety
- Improves quality of care
- Promotes effective communication
- Supports evidence-based practice
- Encourages patient participation
- Provides clear treatment goals
- Facilitates interdisciplinary collaboration
- Improves clinical outcomes
For nursing students, mastering care plan development strengthens critical thinking skills and prepares them for real-world clinical practice.
Need Help Developing a Care Plan?
Creating a comprehensive nursing care plan can be challenging, especially when dealing with complex patient scenarios, multiple nursing diagnoses, and evidence-based interventions. Professional care plan development support can help nursing students and healthcare learners create accurate, well-structured, and academically sound care plans that follow the ADPIE nursing process.
Whether you need assistance with assessment, nursing diagnoses, SMART goals, interventions, rationales, or evaluation sections, expert guidance can help you achieve better academic results while enhancing your understanding of patient-centered care.
Developing a care plan is a fundamental nursing skill that guides patient care from assessment through evaluation. By following the five stages of the nursing process—Assessment, Diagnosis, Planning, Implementation, and Evaluation—healthcare professionals can deliver safe, effective, and individualized care. Understanding the principles of care plan development not only improves patient outcomes but also helps nursing students excel in clinical practice and academic assignments.